
In the United States, it is both hilarious and sad that both major political parties lie and tell citizens that it is possible (in a fiat monetary system) to achieve an ideal trifecta of:
Higher quality medical care
Higher access to medical care
AND we are going to do it all for less cost

This reminds me of that scene in Idiocracy (44:40) when Joe was “so smart” he was given only one week to solve all the world’s problems. Most of the people still interested in politics believe this stuff.If it weren’t for bitcoin, I would not be as honest about my profession as I am about to be. Despite the state narrative to the contrary, savings is freedom. It’s time for somebody to try to be more honest with you.
Why would a bitcoiner want to discuss healthcare?
There are many similarities between the legacy financial system and the legacy medical system. Both money and "modern medicine" are critical tools that should be open source enough to allow people to have fair access to them.
Austrian Economics applies to both systems. Both systems are subject to opportunity cost and scarcity. Both systems are purposely made unnecessarily complicated to disguise the diversion of scarce resources away from paying customers- and enrich entrenched rent seeking middlemen. In both systems, people in suits use excellent manners and virtue signaling to lull customers into a sense of mesmerized trust. In both systems, customers are spending more and receiving less value in return.
Scams are defined as fraudulent business schemes. The fiat monetary system is a scam. The legacy medical system is a scam fueled by the base layer of the fiat monetary system. Bitcoin is monetary truth. Bitcoiners resent scams.
“You don’t know what it is, but it’s there, like a splinter in your mind, driving you mad.”

As a physician who frequents bitcoin Twitter, I'm often frustrated by anti-physician comments that I observe. I get it though. A lot of you feel like you’re being treated like just a number in an uncaring system. Your experience is rapidly devolving into that of being a customer at the state department of motor vehicles. Why don’t your doctors seem to care about you? Why isn't every medical option on the table and being discussed in detail? Why does it seem like they are always trying to get rid of you as fast as possible? Why does it seem like they have been deputized to be enforcers of state policy? How is this all possible in an era of exponential technological advancement?
Here is my attempt to try to answer these questions, based upon my own experience in the American legacy medical system. Another physician might see things differently, or come to different conclusions.I have the great privilege of serving my patients as their physician. I am also stuck working in the horribly inefficient legacy medical system — in which I am finding it increasingly difficult to deliver the highest quality care and/or be fairly compensated for my time.
As doctors, we were taught that our responsibility is to be our patients' greatest advocate. We were supposed to offer the best care plans, regardless of cost. Yes, this did absolutely lead to some waste of resources — but in the past, with relatively primitive technology, our patients received better care. Patients felt like they received better care because providers spent more time with them. We can give patients all the portal website access and smartphone apps in the world, but there is no substitute for our scarce time.
Your doctor probably got into medicine with good intentions. I believe that almost every physician starts his/her medical career with the intention to “help people”, or at the very least with the intention to provide fair healthcare value. It is therefore understandably frustrating for patients that these intentions do not seem to be reflected in actual practice.
Do physicians make too much money? Maybe. I can tell you that it used to be a lot worse. Margins used to be so obnoxious that most physicians (except the extra greedy ones) seemed to have no issue spending extra unpaid time with people who needed it. This was relied upon to assure that those with less desirable insurance plans were well cared for. We have reached the breaking point of that buffer arrangement. Most providers no longer have the luxury of donating unpaid time. Margins are thin to the point that many private (read: unsubsidized) practices are closing.
Contemporary medicine, at least in the United States, is an incredibly regulated and permissioned industry. The saying “bitcoin fixes this” is commonly spouted by sound money advocates. If we desire better healthcare and want bitcoin to be a part of the solution, we need to consider a rather complex web of barriers.
Part 1: Barriers to high quality care within the legacy medical system
Why is it increasingly difficult to deliver high quality healthcare?
In my opinion, state narratives are becoming less logical. Medical credentialing helps to assure that physicians avoid providing any medical advice that contradicts state narratives, regardless of personal educated opinions. It is illegal to practice medicine without a certificate and/or a license. I don't think that people appreciate how disastrous it would be for physicians to make the system angry and as a result lose their licenses.
For example, I spent 9 years in post-graduate training to obtain an M.D. and complete residency and fellowship training. In doing so, I sacrificed 13 years of earning potential (including time for a 4-year college degree), and I paid for the privilege of doing so.
During residency I worked 80-to-100-hour weeks. I was exposed to all sorts of infectious diseases that were objectively more dangerous than the one that most people seem scared of now.
I had to pay for the opportunity to take many tests. I was broke, exhausted, irritable, and boring. My college girlfriend dumped me. If I flunked out of medical school or residency, I would have had no money, no skills, AND a huge amount of debt. My medical school wasn’t shy about threatening to expel those that misbehaved. I had a friend that got suspended for 3 months, because she needed a day off and got caught lying that her grandmother had died (she now works at one of the best hospitals in the country). I know this was a dumb move, but the amount of fear and anger that this incident left me with has never abated. We all took huge risks to get here.
All of this to get certificates that give us permission to participate in medical employment. After this investment, it would be crazy to do something to risk losing the permission certificates. I think it's easy for people who did not put the work in to say otherwise.
Also consider that by spending all this time learning just one thing, physicians tend to have little other trade skills to fall back upon should they lose their permission certificates, and most of us can’t afford to. We tend to be debt slaves. A lot of physicians have nice houses and nice cars, but they don’t have any savings because they haven’t really studied money. Most physicians have no real choice but to comply with the rules and narratives of the system.
Another layer of control via permissioned medicine, involves permission to receive payments from insurance companies. Assuming physicians are not opting out of the legacy medical system and transitioning into a free-market medicine model (part 2 of this discussion), they must be approved by- and enrolled with the various insurance plans.
Insurance plans can fire you if the average cost of your services is too great, or if you are deemed to be somebody who promotes “unapproved” therapies. Insurance plans dictate what tests and therapies will and will not be covered, often completely regardless of medical appropriateness. I often tell patients: “Plan X is the highest quality option, but your insurance plan covers Plan Y.” Patients then almost always choose Plan Y (especially more recently as the population is becoming less wealthy in general).
Frequently, when expensive testing and therapies are absolutely indicated, insurance plans will punish providers by requiring excessive paperwork and phone calls to argue for obvious necessities. This is called “obtaining prior authorizations.”
I recently had a patient who had severe obstructive sleep apnea (stopping breathing to the point of frequent severe hypoxemia) that required >40 office communications to get the insurance company to “authorize” a machine that was necessary (assuming oxygen is necessary) to stabilize the airway. I personally spoke to the insurance company on the phone twice totaling more than 1 hour of my time. The “physician peer reviewer” told me: “Yeah, you are right, but I still can’t authorize treatment because of X red tape.” (If you knew what the specific red tape issue was, the whole thing would seem even dumber).

Physician and staff time for trying to “authorize” payment for care is not compensated. In my opinion, these frequent occurrences are purposeful and designed to slow providers down so we will ultimately cost insurance companies less. It is crazy that there is no mechanism to limit the amount of work an all-powerful insurance company can require from healthcare providers to “authorize” the coverage of necessary testing and therapies.
Prior authorization requirements are different for different insurance companies. Standards are randomly applied by insurance companies. When I order a test or a therapy, I often don’t know if it will be covered by health insurance and/or how much work “authorization” will require of my office. This assures that we cannot have an efficient standard protocol to deliver care. Please understand these barriers result in us having less time to talk to you about things that you care about.
Another layer of control preventing me from personalizing your care is the fact that if I treat you uniquely and things go wrong, then you might become angry with me. People seem to be getting angry more easily. You might sue me. You might write a bad online review (and to the thousands of people that I have helped: would it kill you to occasionally leave a positive review?). You might complain to your health insurance company, or to my hospital.
I need to be conservative, much like the financial advisor that you fired for not recommending bitcoin needed to be conservative. I am safest working within the narrow confines of approved algorithms, whether I agree with them or not.
In a way, my fear of repercussions does keep you safer. This is a double-edged sword though. It also makes it less likely that I will personalize your care, and more likely that I will protect myself by treating you in the exact same way any of my other colleagues would treat you (hint: not amazingly). Fear encourages me to order extra testing, just to be safe. There is some antagonistic doctor-patient dynamic at play.
You might say: “I’m paying more for my health insurance and I’m receiving worse quality care, despite exponential technological advancements. How is that possible?” In large part, this paradox is related to the explosion of administrative middlemen.
A lot of the money spent goes into the pockets of administrators and health insurance executives that don’t provide any direct care.
These executives can do well while medical practices themselves are on the verge of closing. Fortunes are made by those skilled in the shell game of shuffling money around enough to prevent pandemonium, and then skimming what is left from the pot (any money that should rightfully be utilized for direct medical care). Dudes with MBA’s in fancy suits that have a knack for politely skimming money from the pot are not scarce medical resources.
Have you ever noticed that animal hospitals tend to look nicer than human medical offices? Healthcare is not a free market. Insurance companies fix prices, regardless of natural supply and demand. Some insurance companies pay much less than other insurance companies for the same services. The percentage of patients with “good” insurance plans is decreasing. Insurance companies agree to pay hospital systems more money than private practices — for the same services — to support higher administrative costs! Some needed services are no longer worth providing.
Price fixing has resulted in tremendous decreases in reimbursements over the years. My reimbursements have decreased an estimated 20-50% since 2010. In that same period, the USD M1 money supply has increased >8x.
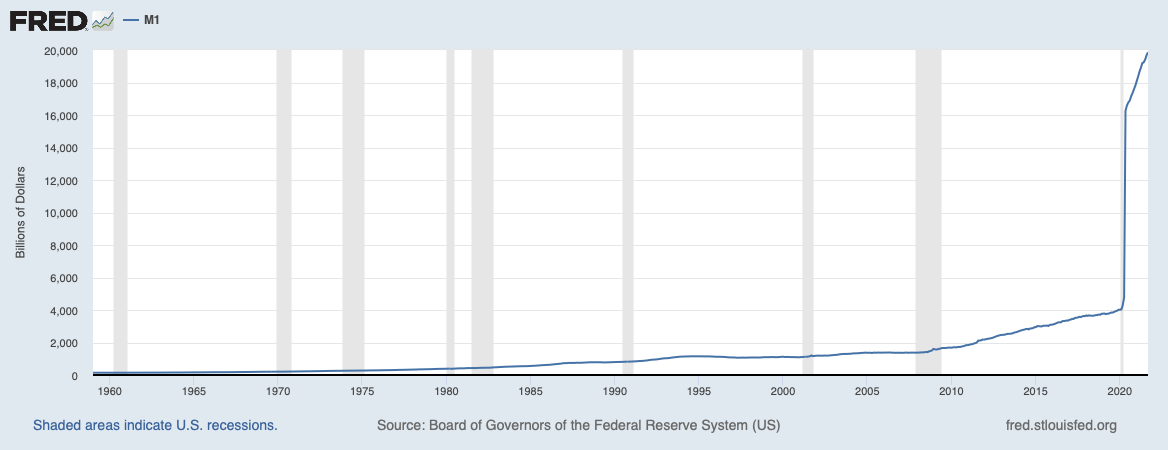
https://fred.stlouisfed.org/series/M1SL#0
Now superimpose reduced reimbursements and increased monetary debasement with increasing overhead costs. Medical clinics have high (and perpetually increasing) “fixed overhead” costs.
Liability insurance
Real estate
Front desk staff
Nurses/clinical assistants
Healthcare benefits
Disability insurance
IT (this is huge in the era of electronic EMR’s which must be “compliant”)
Billing
Accounting
Internet
Phones
Copy machines
Document shredding
Cleaning service
Certificate renewals
Hospital staff membership renewals
“Continuing medical education”
Financing
Payroll processing
Payment processing
Credit card fees
I’m sure that I am missing some items.
Many more patients must now be seen just to break even. Each unit of work is becoming less valuable.
If we are being honest, this means that each patient is becoming that much less important to the bottom line of medical practices. Incentives matter. We need to see more patients and therefore we need to spend less time with each one of you. If you are a “difficult patient,” or a just a complicated patient who may rightfully require a significant degree of attention, your physician cannot afford to have a lot of patients like you. We need a significant portion of patients like you to become dissatisfied enough to find another provider. We need to discharge patients faster if they don’t pay their bills or are rude to the staff (some of you are getting a little crazy). My job is decreasingly focused on keeping you happy.
Who are doctors really serving if each patient’s status is trending towards not being the customer? Who must we keep happy? Sadly, the important parties are increasingly becoming the referring primary care providers, health insurance plans, medical organizations, hospital systems, licensing boards, etc.
At your visit, I have only 15 minutes to:
Talk to you and figure out what is bothering you.
Document a bunch of stuff that doesn’t matter but is required so that insurance companies will pay us. They like to slow us down so our care is less expensive.
Decide upon an appropriate treatment plan.
Figure out what your insurance plan covers.
Superimpose #3 onto #4.
Explain #5 to you.
Document everything in a way that satisfies the insurance company so that they agree to pay for your evaluation and management. This is the most time-consuming step.
These 15 minutes do not even include significant physician time spent after the conclusion of the visit on paperwork to further “authorize” testing and treatments — the rationale of which had already clearly been documented in the clinical note. This does not leave much time for small talk, getting to know you as a person, or exploring any strategy that is outside of normal algorithms, regardless of how reasonable that strategy is. (To make matters worse, in the mask era I don’t even know what half of my patients look like anymore.)
There's not enough time in the day for me to do everything as responsibly as I would like to. I barely have enough time to talk to you and document your clinical note. My physical examinations are not as thorough as I would like them to be. My review of your medical history is not as thorough as I would like it to be. My courtesy calls to you to review results or discuss acute issues are not as frequent or timely as I would like them to be.
I am increasingly forced to prioritize issues and cut corners. This hurts my level of service to you. It puts you at risk and it puts me at risk.
I suppose I could take my work home and improve upon these deficiencies, instead of interacting with my family, exercising, or learning to protect myself with sound money. Why aren't today's doctors as dedicated as prior generations? The simple answer is that the rewards are no longer justifying that sacrifice. Why would I sacrifice health, learning, teaching, and enjoying in order to contribute more to a system that appreciates any level of sacrifice measurably less every month?
I think many people working in other industries can also identify with this sentiment. Know that your doctors are not immune to this because they “took an oath”. I know I sound like a jerk. I’m sorry but this needs to be said so you can try to understand where we are.
I don’t think that most doctors would say this, but doctors are some of the worst virtue signalers that you will ever meet.
I assume doctors that will continue to virtue signal their dedication to a broken system are the ones that can’t see a way out because they have been kept too busy to really study money.
Bitcoiners are fond of complaining about their doctor’s lack of nutrition counseling. A physician could help patients by encouraging them to limit carbohydrates, at least mix in some moderate exercise, avoid smoking, and moderate alcohol consumption. Stop eating sludge. Get off your phone. Go walk around the block. I do think that physicians should talk about these things, but the current incentive structure assures that we lose money by spending any significant time doing so.

One fun example of frustration with non-personalized care was when a bitcoin influencer was surprised that his doctor wouldn’t advise him about hallucinogenic mushrooms. This made no sense to me. There is no financial incentive to spend time straying from algorithmic “medical advice,” and/or accept the obvious liability of talking to people about hallucinogenic mushrooms. While I’m even open to hallucinogens possibly being appropriate in the realm of medical consideration, such action is strictly disincentivized. I’ll also acknowledge that if you are into such things, you know more about them than we do. Our knowledge base is admittedly narrow, because in the current system we are not at all incentivized to become skilled outside of our approved algorithms.
On a local level, the emergence of “Accountable Care Organizations” is helping to assure that physicians remain trapped within the legacy medical system.
“ACOs are groups of doctors, hospitals, and other healthcare providers, who come together voluntarily to give coordinated high-quality care to their Medicare patients.
The goal of coordinated care is to ensure that patients get the right care at the right time, while avoiding unnecessary duplication of services and preventing medical errors.
When an ACO succeeds both in delivering high-quality care and spending healthcare dollars more wisely, the ACO will share in the savings it achieves for the Medicare program.”
What does this really mean?
An ACO is a regional group which utilizes a legal kickback system to generate income by withholding money budgeted for the care of Medicare patients. It uses that cost savings to pay primary care providers supplemental income. It is a capitation reimbursement system for Medicare patients. Each Medicare patient is budgeted for a certain amount of annual cost. At the end of the year, the ACO executives and the primary care providers share in any surplus money.
This system incentivizes primary care physicians to spend less time and/or resources on Medicare patients, with an intention to prevent high-cost testing, treatments, and/or emergency situations.
You might say: “That is insane. Why aren’t people going to jail? Why aren’t people rioting in the streets?”
The ACO system justifies itself by promising patients “quality care.” Therefore, physicians and their staff spend more time documenting proof of “quality care”, leaving less time to actually do the caring. ACO executives profit from this system, AND they also gain control of primary care providers’ extremely valuable referral patterns by “strongly suggesting” that referrals to specialists be kept within members of the system.
Bitcoiners often ask why doctors don’t “accept bitcoin.”
Simply accepting bitcoin for remittances within the legacy medical system is not a game changer at all. One would still have to follow the rules and the time constraints of medical insurances (time is limited by overhead requirements and insurance specified fixed fiat-denominated reimbursements, regardless of medium of exchange).
In fact, accepting bitcoin would require hiring a medical biller and an accountant (these are two separate lines of salary) who are not only skilled enough to navigate within the legacy system, but who also understand bitcoin and bitcoin accounting. These people basically do not exist.
It is hard enough finding people skilled enough at legacy medical system tasks, who are also adaptable enough to navigate the system’s frequent requirement changes, and then manage to keep those people happy within the confines of decreasing profit margins.
Therefore, bitcoin needs to evolve to become seamless before it can be incorporated within the legacy medical system. It needs to reach a point where people are using bitcoin without knowing that bitcoin is being used. Otherwise “accepting bitcoin” within the legacy medical system is next to impossible, and even if a practice manages to equip its system with super-specialized personnel capable of processing bitcoin remittances, it wouldn’t directly improve upon level of service.

Part 2: Barriers to medical providers opting out of the insurance-permissioned legacy medical system to offer patients free market medical choices
I have tried to establish that it is difficult to personalize care and optimize an individual’s medical management within the current system. Accepting this, one may wonder why physicians who are unhappy with the limitations of the legacy medical system don’t simply opt out and see patients in a medical free market?
Wouldn’t it be great if physicians could spend more time with patients, individualize evaluation and management choices, and choose from any testing or therapy, regardless of whether they were permissioned by insurance companies?
Free market medicine could come in the form of concierge medicine, where patients pay a recurring membership fee as a retainer to assure that a physician is available when necessary. It could also be based upon an out-of-pocket a la carte fee for service model. Why don't all doctors offer free market options? Why don’t bitcoiner medical providers provide care to other bitcoiners by accepting fees directly with bitcoin?
It is so much more difficult for a provider to opt into free market medical care than most people realize.
Almost every patient possesses medical insurance. This is both required by law, and practical. One generally would not want to be without medical insurance in case catastrophe occurs. I know that a lot of bitcoiners pride themselves on their healthy lifestyles (I hear a lot of the bitcoin carnivores have huge muscles), but stuff happens.
Patients who purchase medical insurance tend to have the expectation that their insurance will pay for all medical care. It is the rare individual that is willing to pay out of pocket for care that is not covered by the medical insurance system. I find this to be true through a wide spectrum of affluence. I am surprised that even wealthy people tend to make medical decisions based upon that which is covered by their medical insurance plan, regardless of care quality.
The reluctance of patients to pay out of pocket for medical care dramatically limits the population which can be catered to by a free market medical provider. This tendency is worsening as the population’s overall purchasing power decays. Several times per day, patients who have unknowingly been devastated by fiat theft will tell me, “I can’t afford to do that. I am on a limited fixed income.” I sadly express my understanding.
Given a limited target population of patients willing to pay out of pocket for free market medical care, medical providers almost all enroll to have the privilege of accepting payments by insurance companies. When a provider sees a patient with medical insurance (>99% of patients seen in my clinic) there is a rule that the provider is not allowed to charge extra for anything that “is covered” by the medical insurance plan, regardless of whether we agree with the reimbursement amount. We cannot charge for extra time like lawyers typically do. We cannot charge retainer fees. Therefore, if a patient has medical insurance and the doctor is under contract with that insurance, both are effectively excluded from engaging in any type of free market medicine outside of the insurance plan terms.
A bitcoiner might ask: “There are a growing number of wealthy bitcoiners in the world and we now have video conferencing. Why don’t bitcoiner medical providers offer telemedicine services globally to other bitcoiners?” As it happens, there is a geographical control layer. Medical providers must be licensed in the state in which they are practicing. Limiting the patient population to a small geographic area drastically limits the number of patients that can be seen via telemedicine.
If medical providers are also a bitcoiners, then there is a decent chance that they can afford to work part time. Why can’t they just see a limited number of bitcoiner patients who are willing to pay out of pocket in a medical free market? Recall the increasing overhead costs discussed above. Even if overhead cost can be significantly decreased by shedding some of the legacy medical system’s inefficiencies, the cost of running a medical business would remain very substantial. If I don’t see a lot of patients or charge very high fees, I will end up paying for the overhead cost myself so that I can donate my scarce time. It seems like it would be dumb to pay to lose money working.
Revisiting ACO’s, primary care providers who do not enroll with Medicare are left out of the safety net of the ACO kickback system. This disincentivizes primary care providers from leaving the government insurance system. In my area, I estimate that 90% of primary care providers belong to 1 of 2 large ACO’s.
With margins being strained (decreased reimbursement rates, increased overhead costs, fiat loss of purchasing power), most specialist practices would not survive a major decline in primary care referrals. Therefore, specialists also need to be enrolled with both Medicare and the ACO(s). Memberships must be kept in good standing. Failing to assimilate into and comply with these programs would be potentially disastrous and threaten the viability of any medical practice.

Part 3: Healthcare is doomed vs bitcoin is hope
You may come away from this thinking that I am a rather pessimistic person. My medical colleagues, including my physician wife, tend to be much less pessimistic about the current system than me. I am suffering from some physician burnout. I have seen a lot of things I cannot unsee. This is largely just the burden of being a bitcoiner. I think that most of my colleagues are smart people, but most of them exhibit cognitive dissonance that is common amongst those who are relatively successful in legacy systems.
There are people who profit from diverting value away from patients and healthcare providers within legacy medical system. I like to call these people our overlords, because they steal our time, and time theft is slavery. Patients and healthcare providers all suffer at the hands of our overlords.
Who are the overlords? They are the politicians, bankers, Wall Streeters, pharmaceutical executives, health insurance executives, hospital administrators, etc., who suck value from the system that should have been directed towards patients and actual healthcare workers.
These rent seekers profit from various forms of taxation, and ultimately from an inefficient system that must continue to accelerate money printing to avoid grinding to a halt. The overlords benefit from debasing fiat currency more than downstream users (Cantillon Effect). I don’t mean to overly generalize, there are some good people in these industries. I am friends with some overlords. Everybody is acting in their own self-interest. Everybody is a scammer. Don’t hate the player, hate the game. I just wish that the game didn’t reward being a scammer.
We need to fix medicine. It is becoming toxic to work in this industry (not the good kind of toxic). Our ability to provide care is so limited that you could probably replace most of us with free apps right now.
I believe that the only reason this hasn’t happened yet is because the system still needs to have a facade of caring, and AI hasn’t yet progressed enough to pretend to care. It won’t take long for AI to master the appearance of caring.
I really am hopeful. I want to be a positive soul like Phil and Nico (shoutout @Simplybitcoin!). I do think that bitcoin fixes this. I just don’t think that bitcoin fixes this directly or quickly. Medium of exchange is not the problem in the current medical system.
The biggest problems we have in medicine are:
Decreasing wealth of both patients and physicians. Physicians with reduced savings have less ability to donate time that is not strictly compensated. This is a problem in a fixed pricing system when some necessary services are no longer worth performing well. Patients with reduced savings have less ability to opt out of a failing system.
Overregulated permissioned medicine. This limits options, fixes pricing, rewards middlemen, increases overhead, decreases competition, forces compliance with subjective standards, etc.
As fiat continues its inevitable collapse, patients and providers are becoming relatively less wealthy. I believe this is the primary etiology of an increasing trend away from quality care and towards "cost effective" care. My observation is that the more we focus on cost-effectiveness, the more resources we divert to prove that we are being cost effective (we pay more people to assure that we are spending our money wisely). This hurts patients, disincentivizes those directly providing medical care and enriches middlemen.
Bitcoin is a lossless battery for storing time and energy. It is monetary integrity. It is money perfected. “It can’t be bargained with. It can’t be reasoned with. It doesn’t feel pity, or remorse, or fear. And it absolutely will not stop, ever.” (Sorry- that was from Terminator. I got carried away.)
Bitcoin cannot be used to steal from its users, and therefore it can stop systemic fiat theft via inflation and crony capitalism. This allows for both patients and physicians to securely store time, which should improve the wealth problem. This will increasingly give both parties the freedom to opt out of the legacy medical system and into a more free market model of medicine. This in time can reduce the grasp of overregulated, permissioned medicine.
I don’t think that our overlords want providers to have savings. A funny thing happens when savings are achieved. Freedom is increased. Desperation is replaced by honesty. A medical provider that isn't afraid of losing his job is more likely to tell you his true opinions and less afraid to stray from state narratives.
Whether I agree or disagree with somebody, I want them to tell me what they really think. A solvent medical provider is likely to offer increased management options and less likely to order unnecessary testing. With reduced desperation, medical providers are more likely to leave business models that don’t allow for proper patient care.
I don’t think that they want you, the patient, to have savings either. If your freedom is increased and you don’t think that the system is acting in your best interests, you would have an increasing ability to say no and opt out of the system. If you are unhappy with my service and you fire me, I would understand. I want you to have that option. The last thing that I want to do is hang out with 25 people per day who are angry with me.
We aren’t going to reduce the number of administrative middlemen by increasing regulation in the name of “helping people.” The only path to improving care is an increased reliance on the free market, which cold-bloodedly will not allow for these systemic inefficiencies. This will be necessary if we are to allow for efficient allocation of scarce resources.
Well-meaning proponents of fiat-fueled, subsidized, price-fixed medicine (some call this socialized medicine) might ask: “But… in a free market, there will be those who cannot afford to purchase the highest quality care.”
I would respond by saying: “Yes”, which might come off as a little cold, so I would follow that up by saying: “But in today’s increasingly inefficient healthcare system, NOBODY is receiving the highest quality care, and (Michael Saylor voice) by the way, in a sound money system, the less fortunate among us will at least have a fighting chance to start building savings and gain optionality”.
In a medical system built upon a foundation of decaying fiat money, we have a decreasing ability to provide the best care to everybody. Currently, the accepted solution to this problem is, “Leave it up to doctors to determine what level of care is necessary”, but necessary is a subjective term.
If you leave it up to me, I’m always going to say that the absolute best care is necessary, because my role is to act in the best interest of the patient, rather than in the best interest of health insurance companies. It is my hope that we can at least start having honest discussions about this, because the work required to request care that ultimately will not be authorized, and/or virtue signal that we are delivering “quality care” to every patient, is driving inefficiency and worsening the product.
The fundamental question — the elephant in the room that most are unwilling to address — is: "What is our medical system really trying to achieve?"
Are we trying to give our patients the highest quality medical care, or are we content to continue delivering a scaled down "cost effective" version of medicine, and hoping that cutting corners does not kill so many people that it becomes an inconvenience?
If we return to the Utopian healthcare trifecta promised by our various overlords:
Higher quality medical care
Higher access to medical care
AND we are going to do it all for less cost
As stated above, the adoption of bitcoin by individuals and companies can greatly improve the wealth problem for both patients and physicians. This should improve both quality of and accessibility to healthcare.
Reducing the cost of healthcare seems impossible to most. However, this is possible with, and only with, a bitcoin monetary standard. State-incentivized actors tell us that CPI demonstrates that there is only a low degree of purchasing power inflation (note: even low percentage inflation compounds very significantly), when in fact there is a high degree of monetary base inflation (see USD M1 money supply chart above).
In my opinion, the huge difference between these 2 ways of observing inflation is not discussed enough. We should be using increases in base money supply to describe inflation rather than decreases of purchasing power. We now have bitcoin and no longer need to accept inflation, regardless of how we choose to describe it.
We should all be benefiting from natural exponential technological advancements, which should perpetually deliver goods and services that are both of increasing quality and decreasing cost. The fiat system deceives us, and steals the added value of these natural processes from all fiat users. Things that should become less expensive and of higher quality, instead become more expensive and of lower quality. In a sound money system, goods and services, including healthcare, would continuously evolve towards higher quality and lower cost.
There is no simple solution to providing everybody with the opportunity to receive the best medical care. Printing does not fix this. Voting does not fix this.
Bitcoin can increase financial freedom and optionality for both patients and physicians. Bitcoin can reduce the cost of healthcare by delivering the full benefit of natural exponential technological advancements to everybody. As a result, this decreases reliance on the inefficient overregulated permissioned crony scam legacy medical system. It increases free market medical choices and may enable us to salvage a sinking ship for everybody’s benefit. The legacy medical system, like many systems, must be torn down and rebuilt, starting with the foundational base layer of money.
I believe that bitcoin adoption is the only path that can stop the legacy medical system’s race to the bottom.
Bitcoin is hope.
Frito2x is a toxic pleb who is also a double board-certified American physician. He is hoping to share his fiat medicine experience to help people make more educated healthcare decisions and career decisions. He is the host of The Emancipated Plebcast.